Cholesterol plays a variety of essential roles in the body, yet receives a very bad press for contributing to heart disease, while cholesterol-lowering statin medications continue to be heavily prescribed worldwide. Our body produces much more cholesterol than we consume through our diet, so what else is causing the problem?
Types of cholesterol-containing ‘vehicles’
Cholesterol is a waxy, fatty substance produced primarily by the liver and just as oil and water do not mix, neither do waxy cholesterol and watery blood, so cholesterol needs a protective vehicle to surround it and carry it around the body. One of the most important vehicles is low-density lipoprotein (LDL) which transports cholesterol to various cells in the body. Here, cholesterol contributes to the function of cell membranes, including brain cell communication and is also converted to vitamin D and steroid hormones such as cortisol and testosterone. High-density lipoprotein (HDL), another type of transport carrier, removes cholesterol from the blood and takes it back to the liver, to be broken down and excreted in bile.
The liver and digestive system work together to achieve cholesterol balance. 1 If too much or too little cholesterol is built into the membrane of cells, they are unable to function properly and there is an ongoing requirement for cholesterol to be added or removed accordingly. Only the liver can break down cholesterol, therefore it is always important to nutritionally support liver function in individuals with elevated cholesterol.
Cholesterol and heart disease
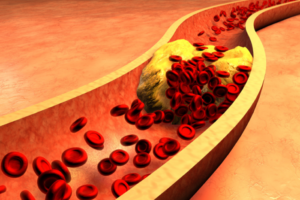 HDL and LDL cholesterol are commonly classified as ‘good’ and ‘bad’ respectively and analysis of blood test results tends to focus around this theme. However, we also need to consider the sub- types of cholesterol, as the size of lipoprotein carrier particle is important and when it comes to LDL or HDL, bigger is better. Small, dense LDL cholesterol particles are more likely to attach to the lining of blood vessels, where they can become damaged (oxidised) and contribute to the build up of plaque, which hardens and narrows the arteries which lead to the heart. 2
HDL and LDL cholesterol are commonly classified as ‘good’ and ‘bad’ respectively and analysis of blood test results tends to focus around this theme. However, we also need to consider the sub- types of cholesterol, as the size of lipoprotein carrier particle is important and when it comes to LDL or HDL, bigger is better. Small, dense LDL cholesterol particles are more likely to attach to the lining of blood vessels, where they can become damaged (oxidised) and contribute to the build up of plaque, which hardens and narrows the arteries which lead to the heart. 2
The risk of developing coronary artery disease is three times greater if levels of small, dense LDL are elevated, 2 while larger, more buoyant HDL particles are associated with reduced risk of cardiovascular disease. 3 Just as we need to consider the size and number of LDL particles, more recent research is highlighting the need to understand that HDL is an important vehicle for carrying various types of cargo around the body, not just cholesterol and in fact, it might be that these other functions are more relevant to our health. 4 For example, HDL vehicles carry fat-soluble vitamins A, D, E and K around the body, of which vitamin E is a potent anti-oxidant and heart-protective vitamin. It also transports  coenzyme Q10 (CoQ10), a hormone-like nutrient which is essential for energy production in cells; particularly important for the function of heart cells; and is involved in managing blood pressure. 4 CoQ10 is widely overlooked, but should always be considered in relation to the prescription of statin medications, because by blocking production of cholesterol, statins also block production of this very important nutrient and it is advisable to take CoQ10 in supplement form alongside these drugs. Common symptoms of CoQ10 depletion are muscle pain and weakness, which by no coincidence, are two of the most commonly reported side effects of statin medication.
coenzyme Q10 (CoQ10), a hormone-like nutrient which is essential for energy production in cells; particularly important for the function of heart cells; and is involved in managing blood pressure. 4 CoQ10 is widely overlooked, but should always be considered in relation to the prescription of statin medications, because by blocking production of cholesterol, statins also block production of this very important nutrient and it is advisable to take CoQ10 in supplement form alongside these drugs. Common symptoms of CoQ10 depletion are muscle pain and weakness, which by no coincidence, are two of the most commonly reported side effects of statin medication.
How can we influence our balance of LDL and HDL cholesterol?
Dietary cholesterol intake
Cholesterol is produced by the body at a rate of up to 1.4g per day, while dietary intake (from cholesterol-containing foods such as offal, meat, seafood, egg yolks and dairy products) makes up around 0.4g per day. 1 Therefore, while we should of course be careful of the type of food we are eating, we need to think about it in the wider context of how the food we eat affects our digestive and liver function, because it is these organs that have a much greater influence on our cholesterol levels than dietary intake of cholesterol. It is increasingly understood that individuals respond differently to dietary cholesterol, with around 25% of the population being classfied as ‘over-responders’ and for whom blood cholesterol levels spike disproportionately in response to dietary cholesterol. 3 However, there are many other factors which affect both the quantity and quality of cholesterol in the body, including genetics, stress, fitness levels and age.
Saturated fat intake
There is ongoing research and debate into whether saturated fat intake is directly linked to cardiovascular disease, with the hypothesis that this type of fat raises levels of LDL cholesterol. When we look into the detail, studies have shown that increased levels of saturated fat in the diet do indeed increase LDL cholesterol, but that this is made up of mostly the larger, more buoyant LDL particles, which are less likely to have a damaging effect on arteries than small dense LDL. 5
What has become clear, is that the results of studies into low saturated fat diets are greatly influenced by what types of food the saturated fat is replaced with and so we come to the crux of the issue. If saturated fat is replaced by polyunsaturated fats (such as the omega 3 fats found in oily fish and certain nuts and seeds), or monounsaturated fats (found in olives and avocado), it can lower both LDL and HDL cholesterol. 6 However, by replacing the calories from saturated fat with carbohydates (particularly refined carbohydrates such as sugar, white flour and white rice), it can lead to a worse cardiovascular profile, with high triglycerides, more small LDL particles and lower levels of HDL cholesterol. 6,7
Carbohydrate intake
When we consume carbohydrates, it triggers the pancreas to produce insulin, which directs glucose out of the blood stream and into cells, to be converted to energy. Excess carbohydrate in the diet leads to excess glucose in the blood and can lead to cells becoming unresponsive to insulin, something we call insulin resistance. Insulin resistance is implicated in the development of both diabetes and obesity and patients of these diseases are more likely to have higher levels of harmful small, dense LDL cholesterol. 2,8 Throughout several studies in which weight loss was induced by very-low-carbohydrate diets, it was observed that LDL cholesterol concentrations did not increase despite the high intakes of saturated fat on these diets. 5,6 This is important to clarify, as carbohydrates fall under several different brackets. Refined carbohydrates, which elicit a high insulin response, are found to increase the level of small, dense LDL, while a high fibre diet is understood to have positive effects on cholesterol levels. 7,9

While elevated cholesterol is obviously a concern that needs to be addressed, it is rather simplistic to focus solely on reducing LDL and increasing HDL using statin medication, as a preventative approach to heart disease. Cardiovascular disease is complex, can develop over time and there are many other factors to consider with regard to the role cholesterol plays in its development, particularly the balance of fats and types of carbohydrate in the diet. At the other end of the reference range, low cholesterol is linked to stroke, depression and suicide, therefore it seems that there is a very narrow band which respresents a healthy cholesterol level. 10,11
Another area which is often overlooked, is thyroid function. If you have a persistently high cholesterol level but eat a healthy diet, you may have an underactive thyroid. Hypothyroidism decreases the speed at which your body uses fats, protein and carbohydrate and cholesterol and triglyceride levels may be increased with even mild hypothyroidism. 12,13
So what should I eat to maintain healthy cholesterol levels?
As always, you should focus on eating a diet that is rich in plant foods, with plenty of antioxidant-rich vegetables, herbs and spices. Oily fish, nuts, seeds, avocado and olive oil are sources of the beneficial fats which help to balance cholesterol levels. Choose your animal protein carefully, as the amount of cholesterol and saturated fat contained in meat is dependent on what the animal was fed. Grass-fed animals tend to have a more beneficial fat profile, while meat from grain-fed animals is higher in saturated fat and cholesterol. Eggs contain cholesterol but also choline, which helps to break down the cholesterol and they are a great source of protein, so enjoy them daily if you wish, but don’t fry them, as the fats the contain are easily damaged by oxidation. Eat plenty of soluble fibre, found in oats, lentils, apples and most vegetables and keep refined carbohydrates and stimulants such as alcohol, caffeine and tobacco, which directly affect glucose levels, to an absolute minimum.
View List of References
1. Cohen D E (2008) Balancing Cholesterol Synthesis and Absorption in the Gastrointestinal Tract. The Journal of Clinical Lipidology, 2 (2): S1-S3. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).
2. Berneis K K, Krauss R M (2002) Metabolic origins and clinical significance of LDL heterogeneity. The Journal of Lipid Research, 43: 1363-1379. [Online] The Journal of Lipid Research (http://www.jlr.org).
3. Kontush A (2015) HDL particle number and size as predictors of cardiovascular disease. Frontiers in Pharmacology, 6: 218. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).
4. Vickers K C, Remaley A T (2014) Thematic Review Series: High Density Lipoprotein Structure, Function, and Metabolism. The Journal of Lipid Research, 55 (1): 4-12. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).
5. Krauss R M, Blanche P J, Rawlings R S, Fernstrom H S, Williams P T (2006) Separate effects of reduced carbohydrate intake and weight loss on atherogenic dyslipidemia. The American Journal of Clinical Nutrition, 83 (5): 1025-1031. [Online] The American Journal of Clinical Nutrition (http://ajcn.nutrition.org).
6. Siri-Tarino P W, Sun Q, Hu F B, Krauss R M (2010) Saturated fat, carbohydrate, and cardiovascular disease. The American Journal of Clinical Nutrition, 91 (3): 502-509. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).
7. Parks E J, Hellerstein M K (2000) Carbohydrate-induced hypertriacylglycerolemia: historical perspective and review of biological mechanisms. The American Journal of Clinical Nutrition, 71 (2): 412-433. [Online] The American Journal of Clinical Nutrition (http://ajcn.nutrition.org).
8. Siri P W, Krauss R M (2005) Influence of dietary carbohydrate and fat on LDL and HDL particle distributions. Current Atherosclerosis Reports, 7 (6): 455-459. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).
9. Harland J I (2012) Food combinations for cholesterol lowering. Nutrition Research Reviews, 25 (2): 249-266. [Online] Cambridge Journals (http://journals.cambridge.org).
10. Holford P (2004) New Optimum Nutrition Bible, Piatkus Books Ltd, London
11. Sansone R A (2008) Cholesterol Quandaries: Relationship to Depression and the Suicidal Experience. Psychiatry, 5 (3): 22-34. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).
12. Barona J, Fernandez M L (2012) Dietary Cholesterol Affects Plasma Lipid Levels, the Intravascular Processing of Lipoproteins and Reverse Cholesterol Transport without Increasing the Risk for Heart Disease. The Journal of Diabetes and Endocrinology, 3 (5): 57-69. [Online] Academic Journals (http://www.academicjournals.org).
13. Rizos C V, Elisaf M S, Liberopoulos E N (2008) Effects of Thyroid Dysfunction on Lipid Profile. The Open Cardiovascular Medical Journal, 5: 76-84. [Online] Pub Med Central (http://www.ncbi.nlm.nih.gov/pmc).